Inflammation in schizophrenia: A question of balance (2015)
In the past decade, there has been renewed interest in immune/inflammatory changes and their associated oxidative/nitrosative consequences as key pathophysiological mechanisms in schizophrenia and related disorders. Both brain cell components (microglia, astrocytes, and neurons) and peripheral immune cells have been implicated in inflammation and the resulting oxidative/nitrosative stress (O&NS) in schizophrenia. Furthermore, down-regulation of endogenous antioxidant and anti-inflammatory mechanisms has been identified in biological samples from patients, although the degree and progression of the inflammatory process and the nature of its self-regulatory mechanisms vary from early onset to full-blown disease. This review focuses on the interactions between inflammation and O&NS, their damaging consequences for brain cells in schizophrenia, the possible origins of inflammation and increased O&NS in the disorder, and current pharmacological strategies to deal with these processes (mainly treatments with anti-inflammatory or antioxidant drugs as add-ons to antipsychotics).
Reviewed in the article are the multiple and interrelated mechanisms that have been suggested as possibly involved in brain cell damage or neurodegeneration in SCHZ. Based on current findings, these possible mechanisms include:
- Microglial activation or increased microglial cellular density.
- Oxidative/nitrosative stress and neuroinflammation
- Uncontrolled activation of the hypothalamic/pituitary/adrenal axis
- Excitotoxicity and disrupted glutamate metabolism
- Mitochondrial dysfunction and energy deficits
- Reduced levels of neurotrophins
- Impaired neurogenesis
- Apoptosis
- Demyelination
- Effects on glucose transport and metabolism
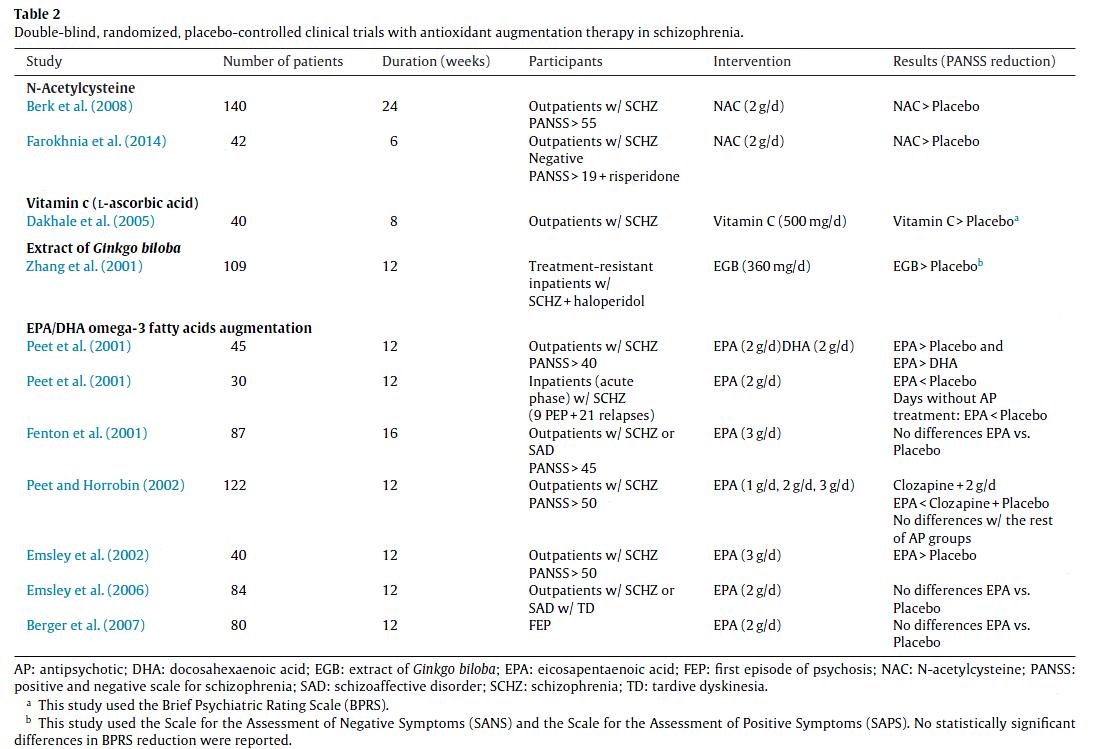
“Augmentation of antipsychotic therapy with antioxidants may an effective and safe add-on strategy in SCHZ patients. Table 2 summarizes double-blind, randomized, placebo-controlled clinical trials with antioxidant augmentation in SCHZ. Other strategies such as vitamin E (Michael et al., 2002) and lipoic acid (Kim et al., 2008) augmentation have shown encouraging results, but in small samples. Besides clinical assessments, it is also important to identify objective markers such as EEG findings to monitor the efficacy of the treatment (Lavoie et al., 2008, Carmeli et al., 2012 and Ballesteros et al., 2013).
If increased inflammation of the brain contributes to the symptoms of SCHZ, reduction of inflammatory status may improve the clinical picture. A recent update has reviewed the randomized controlled trials on efficacy of anti-inflammatory agents in SCHZ, including aspirin, celecoxib, davunetide, estrogens, and minocycline (Sommer et al., 2011). Table 3 summarizes the main double-blind, randomized, placebo-controlled clinical trials with anti-inflammatory augmentation in SCHZ.
Aspirin showed significant effects on the primary outcome (total PANSS score change), while celecoxib, minocycline, and davunetide showed no significant effect. As some of these studies included a small and heterogeneous number of samples, these results should be interpreted with caution. A recent meta-analysis of these studies showed that NSAID supplementation is not superior to placebo in PANSS total score change from baseline, but suggestive effects were observed in studies on aspirin in inpatients and in FEP (Nitta et al., 2013). However, augmentation with acetylsalicylic acid may have the additional benefit of reducing cardiac and cancer mortality in SCHZ (Sommer et al., 2011). Other ongoing clinical trials (FDA, EMA) include combination therapies (add-on antipsychotics) with salsalate, fluvastatin, simvastatin, methotrexate, resveratrol, hydrocortisone, and ibuprofen.
While the focus has traditionally been on antagonizing the proinflammatory pathways, little effort has been made to investigate the anti-inflammatory side of the balance, including stimulation of deoxyPGs or PPARγ activity. Of special interest is the possible use of some thiazolidinediones, potent agonists of PPARγ, widely used as insulin-sensitizing drugs for the treatment of type 2 diabetes (Lehmann et al., 1995). This pharmacological modulation of PPARγ, which may also may directly regulate glutamatergic neurotransmission at the NMDA receptor level (Salehi-Sadaghiani et al., 2012 and Almasi-Nasrabadi et al., 2012), has been suggested as a putative treatment for neurocognitive deficits associated with mood and psychotic syndromes (McIntyre et al., 2006), and it can be considered a multi-faceted therapeutic target due to its anti-inflammatory, antioxidant, anti-excitotoxic, and pro-energetic profile (García-Bueno et al., 2010). However, in a recent pilot clinical trial, the PPARγ synthetic ligand rosiglitazone failed to improve cognitive deficits in clozapine-treated patients with SCHZ, so more evidence is needed to design new trials (Yi et al., 2012).”

“We are still far from having ideally effective and safe treatments to offer our patients. There is therefore a need for a change in the drug discovery strategy, mainly based on a better understanding of pathophysiology (Insel, 2010 and Lewis and Gonzalez-Burgos, 2006). It is still too soon to consider proinflammatory cytokines and/or their signaling pathways a possible novel strategy to treat psychosis (Potvin et al., 2008), although there are already ongoing trials of adjunctive monoclonal antibody anti/pro-inflammatory cytokine therapy (infliximab, tocilizumab) in major depression and SCHZ, whose results could directly implicate inflammation in the pathophysiology of psychiatric disease (Raison et al., 2013 and Miller, 2013). Furthermore, current studies using new anti-inflammatory and antioxidant pharmacological approaches are still in the early stages.”
Interestingly, when given separately to patients with low erythrocyte PUFA levels “EPA and vitamins E+C [can] induce psychotic symptoms in patients… Combined, these agents seem safe.” [1]
See more:
Inflammation and immunity in schizophrenia: implications for pathophysiology and treatment
