Sharing a personal journey in dealing with ‘voices’
Voices in the dark: an audio story | Mosaic
Emerging Perspectives From the Hearing Voices Movement: Implications for Research and Practice
I noted that the initial directions taken by a patient’s psychologist generally resulted in reports of worsened auditory hallucinations and that there may be a better way to approach certain aspects of psychosis – those that are grounded in fear and trauma [1].
“Trauma tends also to be a background factor in psychotic manifestations such as hallucinations. The inner experience of the psychotic episode as well as the encounter with the health-care and law-enforcement systems during the psychotic episode may itself be a traumatic event with post-traumatic sequelae.”
The therapeutic approach experienced by this person seemingly provoked profoundly negative emotional states that were regressive, counterproductive and in the end, likely to lead to maintenance of states of consciousness that were similar to, or worse than the initial presentation. It appeared that when initial trauma/fear memories were reactivated (acutely increasing stress) in the negative affective states that the client was experiencing at the time of therapy, they would reconsolidate adversely – ‘feeding’ the auditory hallucinations and preventing them from successfully attenuating. This is not to totally discount the sustained benefits of continued psychological therapy, which provided some notable improvements over the course of a year.
That said, there seems to be neglect for the appropriate handling of traumatic aspects [such as social defeat, shame [2], ostracism [3], vicarious trauma, interpersonal threat, surviving suicide attempts etc.] which I hypothesise could be better treated using the approach of Hogberg et al.:
This paper reviews the affective neuroscience dealing with the effects of traumatic events. We give an overview of the normal fear reactions, the pathological fear reaction, and the character of emotional episodic memories. We find that both emotions and emotional memories are a tripartite unit of sensory information, autonomic reaction, and motor impulse (the PRM complex). We propose that emotions and movements are part and parcel of the same complex. This is our main finding from the review of affective neuroscience, and from here we focus on psychotherapy with post-trauma reactions. The finding of the process of memory reconsolidation opens up a new treatment approach: affective psychotherapy focused on reconsolidation. The meaning of reconsolidation is that an emotional memory, when retrieved and being active, will rest in a labile form, amenable to change, for a brief period of time, until it reconsolidates in the memory. This leads us to the conclusion that emotions, affects, must be evoked during the treatment session and that positive emotion must come first, because safety must be part of the new memories. In the proposed protocol of affective psychotherapy based on reconsolidation the emotional episodic memory is relived in a safe and positive setting, focused in turn on the sensory experience, the autonomic reaction, and the motor impulse. Then it is followed by a fantasy of a different positive version of the same event. All in all treatment should provide a series of new memories without fear related to the original event. With the focus on the motor program, and the actions, there is a natural link to art therapy and to the mode of play, which can rehearse and fantasize new positive actions.
“Both the negative and the positive emotion must be activated during the treatment session. Activating only negative emotions is counterproductive, because it may lead to a symptom rehearsal that will be consolidated in the memory system as a new negative fear reaction. Thus, it is imperative to start with the positive emotions. The need to activate both negative and positive affects can be associated with the lateralization of emotions in the brain. We suggest that instructions that activate both hemispheres of the brain help in arousing both negative and positive emotions. Activities engaging sensory stimulation such as movement, drawing, listening to music, specifically looking at something, or following a moving object with the eyes are such examples. Presumably they are active to both brain hemispheres.
At first, positive emotions must be accessed. This is needed because positive affect must be part of the new memory to be produced during the session. There should be no activation of negative affect in case positive affect cannot be evoked. In such a case, a longer time and more sessions must be spent to reach a positive affect. Activating positive affect means increasing the parasympathetic tone. This can be achieved by relaxation exercises: breathing and meditation, safe-place imagery, perhaps walking on a treadmill or bicycling on a spinning cycle. Also other aspects of safety in the treatment setting are of importance, such as stage of change process and preferences matching. Once activated, the positive emotion can be anchored in a scene or image with focus on all senses. This means that specific instruction can be given to note the sight, hearing, proprioception, gustatory feeling, and total body sensation in a state of safety and control. After this, instructions are given to connect this positive sensory state with mental clues of retrieval.”
A recent study has found that reconsolidation allows fear memory to be updated to a less aversive level through the incorporation of positive appetitive information.
The impact of acute stress on the regulation of conditioned fear, with details on techniques where stress has been linked to alterations of fear regulation in humans (extinction and emotion regulation) and that of other techniques (avoidance and reconsolidation) are considered in this article.
Therapeutic psychological interventions:
This report from the International Consortium on Hallucinations Research considers the current status and future directions in research on psychological therapies targeting auditory hallucinations (hearing voices). Therapy approaches have evolved from behavioral and coping-focused interventions, through formulation-driven interventions using methods from cognitive therapy, to a number of contemporary developments. Recent developments include the application of acceptance- and mindfulness-based approaches, and consolidation of methods for working with connections between voices and views of self, others, relationships and personal history. In this article, we discuss the development of therapies for voices and review the empirical findings. This review shows that psychological therapies are broadly effective for people with positive symptoms, but that more research is required to understand the specific application of therapies to voices. Six key research directions are identified: (1) moving beyond the focus on overall efficacy to understand specific therapeutic processes targeting voices, (2) better targeting psychological processes associated with voices such as trauma, cognitive mechanisms, and personal recovery, (3) more focused measurement of the intended outcomes of therapy, (4) understanding individual differences among voice hearers, (5) extending beyond a focus on voices and schizophrenia into other populations and sensory modalities, and (6) shaping interventions for service implementation.

“Another trend has been further consolidation of methods for working with voices within the broader context of one’s view of self, relationship with others, and self-narratives that include one’s life experiences. Many voice hearers, especially those who have suffered traumatic events, can experience negative views of self and may additionally see others as potentially dangerous and critical. These views can parallel voice content, making the voice hearer particularly vulnerable to derogatory and threatening content of voices.”
“The potential role of cognitive factors, such as negative self/other evaluations due to traumatic experiences, and responses to trauma, such as dissociation, is ripe for research. However, the literature is at an early stage in operationalizing how to work with trauma when it is associated with voices. Approaches to date have mainly focused on incorporating past experiences into shared formulation, rather than directly targeting trauma-related memories or processes involved in their manifestation in voice experience. Methods such as cognitive restructuring of the meaning of trauma memories, imagery rescripting, prolonged exposure, and eye movement desensitization and reprocessing are beginning to be studied in people with comorbid PTSD and psychosis. This work is important in informing methods of working with the link between trauma and voices specifically. Given proposals that trauma-related dissociative tendencies might confer a vulnerability to voices other areas of potential development might include the application of therapeutic techniques informed by cognitive models of dissociation.”
“As neurocognitive models of voices extend beyond simple models of a core source-monitoring problem, broader cognitive targets may become viable. For example, considering the relation of some voices to previous aversive events and evidence from neuroimaging studies of involvement of the parahippocampal gyrus during auditory hallucinations, a significant number of voices appear to have memory processes implicated in them. Furthermore, there is mounting evidence that social cognition may be important in the experience of voices, and consequently therapies emphasizing interpersonal aspects are likely to be promising. As these mechanisms become better conceptualized interventions may become clearer.”
“…a subtype called hypervigilance auditory hallucination has been described in which there is an exaggeration of the normally adaptive perceptual bias humans evolved to detect threat resulting in auditory “false-positives” from the environment which confirm beliefs regarding feared public exposure of shaming information. Mechanisms here seem distinct from intrusions of self-critical or trauma-related cognition into consciousness. Further development of such clusterings of voice experience and mechanisms is a potential direction in identifying ways of conceptualizing individual differences.”
“A key issue on which participants may vary is the extent to which maladaptive beliefs about voice identity and power predominate, which may apply to only a proportion of people. Potentially this may be most applicable to persons with command hallucinations or threatening voice content, especially those who easily become drawn in to regarding their voices as sentient others. In others the focus may be on derogatory voice content, which may reflect negative self-schemas, or on the intrusiveness of the experience, which may require alternative methods, such as COMET”
“…it is notable that the roots of psychological interventions in cognitive therapy approaches for emotional disorders has meant that therapeutic outcomes for voices have been studied most widely in relation to the emotional consequences of hearing voices (ie, voice-related distress and depression), rather than broader processes of individual adaptation and personal recovery.”
“Processes highlighted by service users as central to personal recovery in psychosis include: developing hope; empowerment and responsibility in self-management of problems; developing a view of self beyond the stigmatized and subjugated role of psychiatric patient; finding new life directions; and social connection.”
⇒ Developing a Compassionate Voice as a Step Toward Living With Voices
A Role for Trauma and Dissociation?
A Community of One: Social Cognition and Auditory Verbal Hallucinations
“…the experience of auditory verbal hallucinations is, for most voice hearers, primarily a social one, with social environment through the lifespan having a specific effect on the presence and form of voices. The fact that most voices are perceived as having social identities with which the hearer interacts in ways verifiably similar to external social relationships suggests that voices often function as internal models of social actors.”
“Furthermore, considering that one of the key experiences of voice hearing is the lack of agentive control over the voices, and that there is a link between social stress, trauma, and auditory hallucinations, the internal social models of individuals associated with intense traumatic or emotional experiences should be less predictable—and resultant imagery more intrusive—than for individuals not associated with such experiences. In addition, recent evidence has emerged that psychiatric voice hearers are much more likely to identify voices as specific living people than non-clinical voice hearers, suggesting that social cognitive factors may differ depending on the level of disability associated with the experience.”
“… it is proposed that problems with the internalisation of social models may be key to the experience.”
Trauma [4]:
“…is any assault to the body or psyche that is so overwhelming that it cannot be integrated into consciousness…an event that shatters belief systems about life…the assumption that the self is sufficiently competent to act, that people are generally good, that the world has meaning and is predictable. Trauma breaches the unspoken contract we think we have with life, that if we do what we are supposed to do we will survive” (MacCurdy, 2007)
“… traumatic events, especially those that are deliberately inflicted by other people, can lead to a loss of “trust” or “confidence” in the world. This undermines the intelligibility of one’s projects, cares, and commitments, in a way that amounts to a change in the structure of temporal experience.”
“…we experience a fundamental assault on our right to live, on our personal sense of worth, and further, on our sense that the world (including people) basically supports human life. Our relationship with existence itself is shattered. Existence in this sense includes all the meaning structures that tell us we are a valued and viable part of the fabric of life” (Greening, 1990)
“He – or she – no longer believes in the very possibility of human connection; he envisages no one who will be present to him and for him if he returns in his mind to the places of horror, humiliation, and grief from which he barely emerged and which continue to haunt him” (Laub, 2001)
Stolorow (2015) describes “two of trauma’s essential features: (1) its context-embeddedness-painful or frightening affect becomes traumatic when it cannot find a context of emotional understanding in which it can be held and integrated, and (2) its existential significance – emotional trauma shatters our illusions of safety and plunges us into an authentic Being-toward-death, wherein we must face up to our finitude and the finitude of all those we love.” He “also describes the impact of trauma on the phenomenology of time and the sense of alienation from others that accompanies traumatic temporality.”
See more: Trauma, Psychosis, and Dissociation
Trauma, Dissociation and Experiential Avoidance [5]
“Patients who hallucinated during the assessment period reported elevated levels of dissociation compared to non-hallucinating patients and healthy controls. Within the hallucinating patient group, auditory hallucinations were significantly predicted by both dissociation and experiential avoidance, although only the effect of dissociation remained significant after controlling for comorbid paranoia. Dissociation predicted the occurrence of auditory hallucinations especially under high stress. Hallucinating patients also reported a greater increase in dissociation in response to minor daily life stress compared to clinical and non-clinical controls.”
“During a traumatic learning situation, conscious memories are laid down by a system involving the hippocampus and related cortical areas, and unconscious memories established by fear conditioning mechanisms operating through an amygdala–based system. These two systems operate in parallel and store different kinds of information relevant to the experience. And when stimuli that were present during the initial trauma are later encountered, each system can potentially retrieve its memories. In the case of the amygdala system, retrieval results in expression of bodily responses that prepare for danger, and in the case of the hippocampal system, conscious remembrances occur.” (LeDoux, 1996)
“Dissociation during trauma inhibits the insula and the hippocampus from binding the memories into cohesive packages, whereas attention to the trauma assists the consolidation of memories. Memory may … appear in extremely vivid bursts with disturbing sensory details, flashbacks, feelings of panic, anger and terror all of which are sudden, intrusive and frightening because they seem to come from nowhere and can’t seem to be regulated in conceptual-autobiographical self-awareness. …It is as if the traumatic event is “locked inside” because the unrealized urges—the failure to be able to act as one would have expected—which have not been integrated… are in a sense holding the neural network hostage” (Fogel, 2009)
“Neuroimaging studies have linked auditory hallucinations to functional and structural differences in speech and language areas—most notably the superior and middle temporal gyri and the inferior frontal gyrus (Broca’s area). In addition, a wider network of non-sensory areas is implicated. These include areas typically described in the auditory verbal hallucination literature as linked to cognitive monitoring—namely, the dorsolateral prefrontal cortex, anterior cingulate, and cerebellum—and areas typically linked to emotion and affect regulation—namely, the anterior insula, hippocampal and parahippocampal regions, and the orbitofrontal cortex . However, these areas typically described as monitoring and emotion areas are also key components in social neurocognitive networks that make up the ‘social brain'” [6]
The dissociated content may be brought into embodied self-awareness:
Any therapy that does not bring the client to conscious self-awareness is incomplete for healing trauma. Embodied self-awareness “is the ability to pay attention to ourselves, to feel our sensations, emotions, and movements online, in the present moment, without the mediating influence of judgmental thoughts…” (Fogel, 2009)
Fogel delineates the restorative nature of embodied self-awareness:
“It allows us to feel ourselves without suppression and yet stay in an emotionally safe zone; it engenders self-trust and the ability to respond appropriately and effectively in current situations; it helps us make choices true to our own needs and values and also use others as resources; it’s a requirement for creativity and engagement. Furthermore, this ability to be our true selves opens interpersonal and spiritual dimensions of compassion, forgiveness and gratitude” (Fogel, 2009)
In order to deal with the past, traumatised people need to activate “…their capacity for introspection. Therapy needs to help them develop a deep curiosity about their internal experience. This curiosity is essential in learning to identify their physical sensations and to translate their emotions and sensations into communicable language – communicable, most of all, to themselves” (Ogden, 2006)
Subtyping AVHs:
Attempts at subtyping auditory verbal hallucinations provide some theories relevant to to the above hypothesis, concluding that “…trauma-based AVH may form a distinct transdiagnostic AVH subtype.” [7]:
“AVH models based upon negative automatic thoughts found in depression, obsessive-like intrusions associated with obsessive-compulsive disorder (OCD) and trauma-related intrusions associated with Posttraumatic stress disorder (PTSD) have previously been proposed to explain the origins/maintenance of AVH. Clinically, the fit of each of these models appears variable from person to person, suggesting that each may represent a distinct AVH subtype. First, some people experience derogatory voices with ego-syntonic content associated with dysphoria, consistent with a model of voices as verbal representations of negative self-schema in the same way that self-critical negative automatic thoughts in depression are seen to arise from the activation of negative beliefs about the self. Second, others experience repetitive intrusive, ego-dystonic voices that are associated with anxiety, disavowed and resisted, potentially giving rise to compulsive behaviors. This is akin to the distressing, repetitive ego-dystonic intrusive thoughts classed as obsessions in OCD. Third, other voices are identical or thematically related to memories of trauma. Intrusive, vivid memories of trauma play a central role in cognitive models of PTSD where failure to adequately process trauma memories results in repeated, intrusive memories, and AVH related to trauma could be similarly conceptualized. Problematically though, the reliving of traumatic experiences in PTSD is usually visual, sometimes olfactory but rarely auditory verbal. Furthermore, while some memory-based AVH may be the result of dissociative processing during trauma, others may be created through bottom-up activation of neural circuitry associated with verbal memory, not being identified as memories due to context memory deficits.
Basing AVH subtypes in cognitive models of anxiety and depression could lead to subtype-specific interventions. Depressive thoughts and feelings are maintained through rumination, and compulsive behaviors through metacognitive beliefs about obsessions. Processes relating to depression and anxiety studied in relation to AVH (eg, rumination and metacognition) may inform future psychological interventions for specific AVH subtypes. For example, because trauma-related cognitions in PTSD are maintained by avoidance and safety behaviors, this offers a psychological strategy for intervention with AVH, as do other techniques from PTSD such as EMDR.”
“Phenomenologically, there is good evidence for a AVH subtype rooted in memories. These voices, if rooted in highly traumatic events, or in frequent adversity in which the same themes or criticisms were repeated many times with minor variations, may be verbatim replays of what was said. However, given the reconstructive aspect of recall and the tendency to create gist memories, voices may not reflect exactly what was said at the time of the trauma. Based on cognitive models, memory-based AVH may be subdivided into 2 types. Both may evolve over time into more extended, elaborated, novel inner speech–based AVH subtypes.
Dissociative.
It has been proposed that a risk factor for PTSD is reduced hippocampal processing of the traumatic event, either because of a preexisting vulnerability or as a response to the intensity of the event. Hippocampal processing would normally integrate information about the event within a spatial and temporal context. In contrast, decontextualized processing of traumatic events could lead to fragmented, dissociated memories of the trauma with sensory properties, intrusively entering into consciousness as AVH. These could be seen to relate to the trauma psychosis subtype previously noted. At a neurological level, as with trauma memories, these may be conceptualized as involving altered functional connectivity between areas such as the amygdala and hippocampus. These could be treated with trauma-informed psychotherapies and/or EMDR.
Nondissociative.
Memories of speech, which have been processed in a normal (ie, nondissociative) manner, may also intrude into consciousness. These may be experienced as AVH due to deficits in context memory causing them to be experienced as current perceptions rather than memories.”
Breggin (2015) details ‘negative legacy emotions’, offers some insights and lays foundations for a trauma-related etiology of hallucinations:
“Hallucinations share many qualities with guilt, shame, and anxiety, including a seemingly involuntary hold over individuals, making them compliant with them. Painful or disabling hallucinations are driven by guilt, shame, or anxiety. Rather than viewing hallucinations as essentially pathological or abnormal, this article examines them as a natural part of a continuum of the human creative imagination that are especially vulnerable to being overwhelmed by traumatic experiences and the resultant amplification of negative legacy emotions. These insights can help to liberate individuals from their psychotic and hallucinatory experiences to live by more rational and loving approaches.”
“In a state I described as psychospiritual overwhelm, they [people with schizophrenia] lapse into helpless with fragmented thinking and communicating. In this study, I relate their hallucinatory “broken poetry” to my new theory of negative legacy emotions. I show that their poetic metaphors and illusions in the form of painful or self-destructive hallucinations are expressions of guilt, shame, and anxiety, emotions that do have primitive origins in biological evolution and early childhood, and that this understanding can help in their recovery from self-defeating, disabling emotions.”
“Negative legacy emotions feel like they are very personal. When one feels guilty, one believes oneself to be bad. When one feels ashamed, one thinks himself or herself to be worthless or to deserve rejection. When one feels anxious, one believes, for that moment, that one is helpless or even doomed. As I describe in Guilt, Shame and Anxiety (Breggin, 2014), none of this is true. Because these emotions were built in by biological evolution and then stimulated and shaped in childhood before the age of reason or even recollection, they can be viewed as having little or nothing to do with who one really is, and in particular, with one’s positive capacities for reason, creativity, and love.”
“…incapacitating human emotions are driven by early childhood trauma and stress, often compounded by losses or abuses in adulthood, and do not originate or emanate from considerations of our place in the universe or mortality. To the contrary, we tend to struggle with existential issues such as the meaning of life after becoming helpless in the face of guilt, shame, and anxiety, and consequent deterioration of our social relationships.”
“Psychotherapists sometimes encourage their clients to own these emotions and even to look for something they may have done to stimulate their guilt or shame. The theory of negative legacy emotions suggests that this approach in therapy is misguided and harmful. It is far more liberating and empowering to view these emotions as primitive, prehistoric relics of humanity’s evolutionary and childhood past that should be seen as alien and of no worth in people’s mature lives. While working on rejecting them, people can triumph over and transcend them with positive values including rational personal responsibility and a joyful approach to life.”
Auditory Verbal Hallucinations as a Dialogical Experiences:
“One important facet of the dialogical approach is that the self is described in terms of space and time. The I changes from one position to another, each one with its own perspectives or voices, which can maintain different relationships with each other based on discrepancy, agreement, opposition, cooperation, etc. This process of continuous positioning and repositioning occurs depending on situational circumstances and exchangeable requirements. The voices of those I-positions express their particular point of view and have their own stories to tell, created with regard to others. Several voices express their view of reality and together construct a narratively structured self. The I not only moves among several points of view, but also among different time perspectives. One may return to a particular moment in the past or have a vision of the self in the future. Imagination enables us to experiment with different imagined and even unreal experiences.”
“The voices of each of the I-positions are related to each other, and this exchange modifies the self system. New interpretations of life experiences may be created as a result of such confrontation. When two or more positions confront each other in discussion, negotiation, cooperation, etc., the self-system may become altered, and the distances and relationships in the dialogical space may also change. Therefore, innovations may come about in the system, for example, a new I-position may appear, or a position that was originally secondary may become important. When the voices come to an agreement, they may merge into a coalition of voices, and a new subsystem may be formed. The positions that become dominant may have more impact on self-control”
“An essential element in these dialogues would be the use of pronouns in second and third person depending on the position each occupies in that mental space.The person not only “hears” his voices, he speaks to them, argues, makes friends with some of them and fights with others, and furthermore, his relationship with them organizes his life, accompanies him and controls his behavior. None of this impedes, different dialogical organizations from appearing, among which, in our opinion, it is very common for one of the positions to dominate, and rigidly and inflexibly organize most of the others, in an attempt to maintain a sense of personal identity which the other I-positions contradict.”

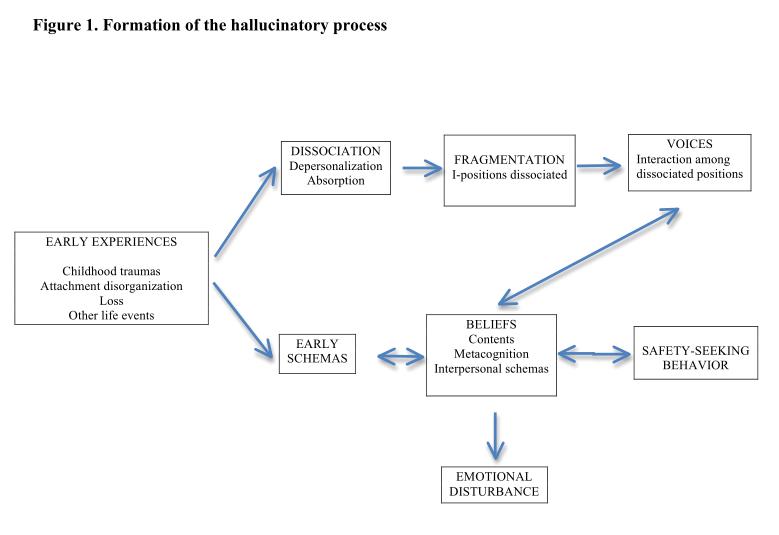
“When the process has been formed and completely consolidated, it is unnecessary for the traumatic conditions and stress that began it to exist for voices to appear. Once the first voice experiences have appeared, and especially, when they have acquired pragmatic and dialogical properties, the subject is completely familiarized with them and they can probably appear and reappear any number of times without the necessity for an intensely stressful event to trigger them. That is, stressful events may be sufficient for the appearance of episodes, but not necessary for them. In this sense, we propose that what facilitates the start of a voice episode is the activation of intense states of absorption, which consist of the appearance of high levels of self-focused attention and imaginative overinvolvement, which together with a loss of metacognitive perspective of the different I-positions, facilitates their becoming distanced from each other. In these states of absorption, the dissociated I-positions acquire their own perspectives of reality and their own narratives, which, depending on the interpersonal schemas acquired by the person during his life, will facilitate the establishment of relationships among them which are very similar to those given to that person and his peers in his daily life. The type of relationship with the voices conditions the formation of beliefs about them on one hand, and on the other, the safety-seeking behavior the person will use to face the supposed dangers associated with those relationships. From this perspective, the emotional disturbance associated with voice episodes are related to beliefs about the voices.”
“…we drop the perspective of the voices as hallucinations and perceptions without external object and concentrate on conceptualizing them as states of consciousness in which different I-positions become dissociated. These positions usually come into conflict with each other, and the person lives them as real experiences undergone at that moment. We think that this theoretical framework is compatible with psychological research done to date on this subject, and furthermore, contributes a functional perspective to the study of voices that makes it possible to understand facets of its phenomenology”
Dysfunctional Schema Modes as Dissociated States and Opportunities for Intervention [8]
“Viewed in a different way, a dysfunctional schema mode is a facet of the self involving specific schemas or schema operations that has not been fully integrated with other facets. According to this perspective, schema modes can be characterized by the degree to which a particular schema-driven state has become dissociated, or cut off, from an individual’s other modes. A dysfunctional schema mode, therefore, is a part of the self that is cut off to some degree from other aspects of the self.
Different parts of the self have split off into separate personalities that are often unaware of each other and that may have different names, ages, genders, personality traits, memories, and functions.”
Beliefs about Voices and Schemas about Self and Others in Psychosis
“…there was a general pattern in which negative-self schemas were more widely associated with beliefs about voices than were negative-other schemas. Negative self-schemas were linked to malevolence, loss of control and metaphysical beliefs in addition to omnipotence, although the relationships with malevolence and negative metaphysical beliefs were no longer significant when partialing out variance shared with omnipotence. The association between omnipotence and negative-self concurs with findings by Birchwood et al. that the rated power and status differential between self and voice is associated with appraisals of one’s own relative power and status in the social world. The metaphysical and loss of control scales have been found to be associated with intolerance of uncertainty, but have not otherwise been significantly studied. Finding an association with negative-self schemas suggests a potential broader relationship with negative self-evaluative beliefs.”
“…general schemas influence the formation of not only appraisals of voice social rank and power (e.g. omnipotence), as has been previously demonstrated, but also those of voice intent (e.g. malevolence) and metacognitive beliefs about voices (e.g. fears of loss of control). This provides a means of accounting for observed individual differences in adaptation to hearing voices: the person’s broader schemas influence the extent to which they interpret the phenomenon of hearing voices as a personal or social threat, in turn impacting upon adaptation and distress.”
“Clinically, identifying schematic beliefs related to beliefs about voices potentially provides an additional therapeutic target for psychological intervention. They may provide a parallel focus of intervention, or an alternate target when beliefs about voices are held with too strong conviction to provide a workable focus. Schemas associated with malevolence may be particularly important in providing a potential target for cognitive restructuring because no trials of cognitive-behavioural therapy (CBT) for psychosis that have included voice malevolence as an outcome have observed changes in this dimension. Indeed, even though malevolence beliefs are robustly associated with distress, methods for working with these beliefs have not tended to be included in descriptions of CBT, which primarily focus on modifying beliefs about voice power, and control over the experience and the origins of voices. Beliefs in voice malevolence are not easy to directly modify into an alternative belief without either colluding with the idea that voices are sentient others, or challenging the person’s overall explanatory model. Hence schemas that may be supporting these beliefs about voices represent an important alternate avenue for intervention. In addition to traditional cognitive restructuring methods, methods of working with voices are emerging that adopt a more experiential approach, which may be well-suited to intervening at a schematic level. Other suitable approaches include methods from acceptance and mindfulness-based therapies that can defuse the impact of negative self-related ideation, and methods described for working with voices in a broader interpersonal context. Further study on identifying the specific content of schemas associated with voice beliefs may inform more precise targets of these developing interventions.”
Examples of Maladaptive Coping Responses:


“…the goal of treatment is to increase conscious control over schemas, working to weaken the memories, emotions, bodily sensations, cognitions, and behaviors associated with them.”
“Unless it is corrected, the schema will perpetuate itself.”
“A dysfunctional schema mode can be described in terms of the point on a spectrum of dissociation at which this particular mode lies. To the degree that an individual is simultaneously able to experience or blend more than one mode, the level of dissociation is lower.”
⇒ A Client’s Guide to Schema Therapy
Potential modifications to “Avatar Therapy“?
Step 1: Validation and normalisation of the patient’s experience
“By assisting the patient to create their avatar the therapist accepts the validity of the patient’s experience and shares in it. This ameliorates the sense of being an outcast or freak.”
– when asked about the worst aspect of hearing persecutory voices, many people say ‘the helplessness’
– people who are able to establish a dialogue with the ‘voice’ feel much more in control
Step 2: Substituting a human figure for an invisible entity ‘voice’
Step 3: A safe space is made available
Step 4: Gaining control over the avatar
Step 5: The avatar changes its persona
Step 6: Linking the patient’s low self esteem with the abuse from the voices
“the avatar linked the abusive voices with the trauma they had experienced”
– “the voices say what you think about yourself.”
– valued aspects of the self are highlighted and the whole sequence in which the patient is faced with these valued aspects of the self challenges their negative view of their nature.
Step 7: Reintegrating the persecutory voice in a helpful, pro-social and adaptive manner
Allows for the embodiment of dissociated content and places the client in control of positive behavioural change.
“An important component of the therapy is that after the first two or three sessions the avatar is made to cease being abusive and controlling, and becomes increasingly supportive of the patient, complimenting them on their achievements, suggesting ways in which they could improve their life, and praising their good qualities. In accord with this change in character, the avatar’s expression is altered to appear friendly and smiling. This may be appraised subconsciously by the patient as a substitution of a loving parent/other for a punitive, denigratory, or neglectful one, enabling them to reintegrate the projected unacceptable part of their internal world into their psychic structure. In a similar vein, Garrett and Turkington (2011) argue that CBT provides a technique to bring “thing presentations” (thoughts or feelings experienced as an external perception) back within the boundary of the self.
As the avatar becomes less dominating and the therapist encourages the patient to be increasingly forceful in opposing it, the patient gains confidence in their power. Hayward and colleagues (2011) have reviewed the evidence that the degree of perceived dominance of the voices directly reflects the patient’s subordinate position in relation to their social contacts. Being low down in the social pecking order may derive from the patient’s treatment… Avatar therapy, by enabling the patient to achieve control over their avatar, leads to a reduction in their feeling of helplessness and enables them to face their actual persecutor with increased courage and boldness.”
Acceptance as a strategy:
“The social demand for reason giving and the practical utility of human symbolic behavior draws the person into attempts to understand and explain psychological events even when this is unnecessary (Hayes, 2002). Contact with the present moment decreases as people begin to live ‘‘in their heads.’’ The conceptualized past and future, and the conceptualized self, gain more regulatory power over behavior, further contributing to inflexibility. For example, it can become more important to be right about who is responsible for personal pain, than it is to live more effectively with the history one has; it can be more important to defend a verbal view of oneself (e.g., being a victim, never being angry, being broken, etc.) than to engage in more workable forms of behavior that do not fit that that verbalization. Furthermore, since emotions and thoughts are commonly used as reasons for other actions, reason-giving tends to draw the person into even more focus on the world within as the proper source of behavioral regulation, further exacerbating experiential avoidance patterns. Again psychological inflexibility is the result.” [9]
A “mindful” strategy to gain greater prefrontal management of limbic responsiveness that involves a change in our language. Rather than saying, for example, “I am sad”, the self-talk that provides more separation between the self and the emotion would be “There is a feeling of sadness right now.” Placing the emotion as an objectively observable phenomenon that is apart from the “observing self ” elicits a greater sense of control over what would otherwise be an immersive emotional experience. [link]
See: Third-wave strategies for emotion regulation in early psychosis: a pilot study (2015)
- Voice hearers may be able to develop a more equal, and thus less distressing, relationship with their voice by improving their perceived social rank relative to others. This may be achieved through assertiveness training, social skills training and/or self-esteem work.Cognitive behavioural therapy techniques can be instrumental in helping an individual to consider the beliefs they hold about their voices and the way in which they respond and relate to them.Addressing how past traumatic experiences have influenced the voice hearer’s relationships with others and their voices in therapy is recommended. [link]
- Cognitive processes found to be associated with depression across the groups were negative schematic beliefs about the self, experiential avoidance and rumination, but not autobiographical memory or problem solving.A number of cognitive factors also predicted the persistence of persecutory delusions, including negative schematic beliefs about the self, worry, and problem-solving difficulties. [link]
- “Therapeutic processes start from the development of a safe and enriched environment to activate positive approach motivational schemata utilising a bottom-up neurological approach, and proceed from a top-down approach to facilitate long-term change in neural architecture.Maintaining arousal within the window of tolerance ensures integration of top-down and bottom-up processing while keeping the social engagement system “online”. When the window of tolerance is narrow, as can often be the case with those who have experienced trauma, there can be a tendency to move into a hypo- or hyperaroused state in reaction to stimuli that activate implicit traumatic memories. In such states there is reflexive defensive reacting, rather than prefrontally mediated integrative and flexible responding to the stimuli. Rapid oscillations between hyper- and hypoarousal can take place in a desperate attempt to achieve regulation—a situation that has been likened to a “biphasic rollercoaster”.
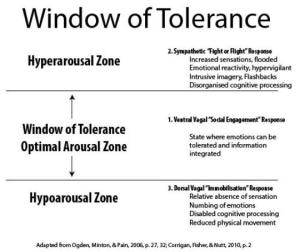
From a neuropsychotherapy perspective, the importance of widening a client’s window of tolerance, especially in the case of trauma, becomes a central goal. Achieving this will increase a capacity to tolerate and integrate thoughts and feelings and keep the ventral vagal social engagement system operative.The implicit emotional memories (procedural memory) known to contribute strongly to motivational schemata are formed in the presence of strong emotion and stored in subcortical implicit memory circuits where they prove to be exceptionally durable. However, when such memory is activated and enters a liable state—a temporarily deconsolidated state or “reconsolidation window” that is opened up via a “mismatch” condition and lasts from four to five hours – it can be radically unlearned. The opportunity to interrupt or modify memory in this way has obvious implications for psychotherapy, especially in regard to those memories that make up core motivational schemata. This “discovery of the brain’s ability to delete a specific, unwanted emotional learning, including core, non-conscious beliefs and schemas, at the level of the physical, neural synapses that encode it in emotional memory” can lead to the complete and permanent elimination of psychological symptoms.The feeling of safety within the therapeutic dyad is of fundamental importance to attenuate the destructive stress responses described above and to take advantage of controllable incongruence as a mechanism of change. A client who is held in a space of trust and security and can engage within their window of tolerance will be able to take advantage of the brain’s natural neuroplasticity.Research has shown that “a safe, enriched environment actually facilitates the development of new neural patterns, which, in turn, leads to enhanced attachment and control, and stress reduction. Psychotherapeutic approaches that provide safe environments will thus enhance the positive social interaction that is an essential element of healthy neural proliferation”. To establish such a safe environment requires a down-regulation of avoidance motivational schemas that may be activated. This is essentially a bottom-up approach of dealing with the physiological stress response before being able to facilitate effective neural change and proliferation. The affectively focused right brain-to-right brain therapeutic relationship, mediated via so-called “mirror neuron” activity, can be effective at establishing safety for a client by down-regulating limbic reactivity and communicating an empathic, supportive relationship that satisfies the basic need for attachment.A safe therapeutic relationship creates the ideal environment for facilitating neural proliferation in an integrative manner, as the nervous system is essentially a social-centric system that thrives on interpersonal love, acceptance, and security.” [link]Other factors:
- Insight reconfigures hippocampal-prefrontal memories [link]
- There may also be extinction resistant changes in the human auditory association cortex following fear/threat learning [link]
- An augmented form of extinction that replaced, rather than merely omitted, expected fear/threat outcomes with novel nonthreat outcomes, with the goal of reducing postextinction return of defensive behaviors, has therapeutic potential. [link]

Pharmacologically Enhanced Therapies
Also of interest is utilising pharmacological options to disrupt fear/trauma memory reconsolidation. One approach which has been extensively researched is the use of propranolol. This may be an effective line of investigation when it is not possible to sustain the prior positive affect required in the Hogberg et al. approach detailed above.
Disrupting Reconsolidation of Fear Memory in Humans by a Noradrenergic β-Blocker.
High Trait Anxiety: A Challenge for Disrupting Fear Memory Reconsolidation
D-cycloserine (DCS) also shows promise.
D-Cycloserine as an augmentation strategy for cognitive behavioral therapy of anxiety disorders.
⇒ EXTINCTION VS RECONSOLIDATION

A recent article describes how “therapies may be optimized for the individual based on the patient’s age, genetic profile and personal history to move from standard treatment of care to personalized and precision medicine.”
“…collectively, our findings thus far point to developmental stage, personal history and heritability profile as factors that can mediate a given individual’s capacity to efficiently and adaptively regulate fear expression. Mechanistically, this can be attributed to a lack of top down regulation of amygdala output by prefrontal regions. In addition, extinction learning does not persistently attenuate fear. Fear responses often return after extinction (Bouton, 2004). Finding alternative interventions that potentially bypass prefrontally mediated fear regulation may be beneficial for attenuating fear memories in populations with diminished extinction learning. One such alternative relies on reconsolidation update, an approach based on the principles of memory reconsolidation.
Dębiec and Ledoux (2004) showed that intra-amygdala and systemic infusion of beta-adrenergic receptor blocker propranalol (non-toxic and safe in humans) could disrupt fear memory reconsolidation in rats. This finding was recently extended to humans using systemic treatment (Kindt et al., 2009). In this study, participants who received propranolol prior to retrieval of a conditioned fear memory showed persistent attenuation of fear response on a subsequent fear recovery test (but see Schiller and Phelps, 2011).”
On the contrary, there are multiple negative results, one review concluding “we failed to find pharmacological blockade of traumatic memory reconsolidation”
Schizophrenia patients may have impaired PFC functionality, hence making informed reconsolidation therapies potentially preferable to exposure-based techniques that are prefrontally mediated:
“… reconsolidation update is a method of fear regulation that is independent of the prefrontal cortex. This makes it a potentially attractive alternative to extinction for adolescents, a developmental group characterized by protracted development of prefrontal regions upon which successful extinction is dependent (McCallum et al., 2010). It may also be helpful for individuals with diminished learning due to genetic and environmental factors, who may not respond well to exposure-based therapies that presumably rely on prefrontally mediated regulation of fear.”
The earlier article also provides framework for therapy:
“…studies have shown that reactivating a conditioned stimulus opens a temporal window during which a fear memory becomes labile and prone to disruption. Extinction during this window leads to enhanced attenuation of fear memory. In therapeutic terms, this approach may already be in use in the clinic without explicit knowledge for why CBT may work for some patients or in some contexts or by some therapists and not others. For example, once identifying the triggers for anxiety in a patient the therapist subsequently meets with the patient. When the patient comes into the office, the clinician may remind the patient of why they are there (activation of a fear memory by presentation of an isolated retrieval cue). Then the clinician builds a rapport with the patient on what may be going well or what puts him/her as ease for at least 10 min (i.e., waiting for the reconsolidation window) before beginning desensitization (i.e., extinction during the reconsolidation window). This approach could be translated into a three-step clinical protocol whereby a clinician would: (1) reactivate a patient’s traumatic or fear memory; (2) engage the patient in an unrelated, nonthreatening activity for 10–15 min; and then (3) initiate the exposure therapy session. This could lead to enhanced or persistent attenuation of the fear/trauma.”

Model for the neurocircuitry of fear regulation in humans through extinction, cognitive regulation, active coping, and reconsolidation. A network of structures including the amygdala, hippocampus, vmPFC, dlPFC, and the striatum are involved in the regulation of conditioned fear expression. The lateral nucleus (LA) of the amygdala receives afferent sensory input and is the site of CS–US plasticity during fear conditioning. The LA projects to the central nucleus (CE), which has outputs to regions that control the expression of the CR. Projections from the hippocampus to the basal nucleus (B) of the amygdala process contextual information during conditioning, and may gate fear expression through the CE. During extinction learning and consolidation, inhibitory connections between the vmPFC and the intercalated (ITC) cell masses are established. During extinction recall, these connections inhibit fear expression through projections to the CE. Inhibitory connections between the vmPFC and the LA may also regulate fear expression during extinction recall through the CE. Contextual modulation of extinction expression is mediated by projections from the hippocampus to the vmPFC and/or LA. During cognitive regulation, the dorsolateral prefrontal cortex (dlPFC) regulates fear expression through projections to the vmPFC, which in turn inhibits amygdala activity. During active coping, information from the LA is routed not to the CE, which drives fear expression, but to the B, which in turn projects to the striatum. The striatum is thought to reinforce instrumental action taken during escape-from-fear or avoidance learning. Reconsolidation diminishes conditioned fear expression through alteration of the original CS–US association stored in the LA. [Source]
Recent studies have highlighted other strategies:
Pathological fear and anxiety are highly debilitating and, despite considerable advances in psychotherapy and pharmacotherapy they remain insufficiently treated in many patients with PTSD, phobias, panic and other anxiety disorders. Increasing preclinical and clinical evidence indicates that pharmacological treatments including cognitive enhancers, when given as adjuncts to psychotherapeutic approaches [cognitive behavioral therapy including extinction-based exposure therapy] enhance treatment efficacy, while using anxiolytics such as benzodiazepines as adjuncts can undermine long-term treatment success. The purpose of this review is to outline the literature showing how pharmacological interventions targeting neurotransmitter systems including serotonin, dopamine, noradrenaline, histamine, glutamate, GABA, cannabinoids, neuropeptides (oxytocin, neuropeptides Y and S, opioids) and other targets (neurotrophins BDNF and FGF2, glucocorticoids, L-type-calcium channels, epigenetic modifications) as well as their downstream signaling pathways, can augment fear extinction and strengthen extinction memory persistently in preclinical models. Particularly promising approaches are discussed in regard to their effects on specific aspects of fear extinction namely, acquisition, consolidation and retrieval, including long-term protection from return of fear (relapse) phenomena like spontaneous recovery, reinstatement and renewal of fear. We also highlight the promising translational value of the preclinial research and the clinical potential of targeting certain neurochemical systems with, for example D-cycloserine, yohimbine, cortisol, and L-DOPA. The current body of research reveals important new insights into the neurobiology and neurochemistry of fear extinction and holds significant promise for pharmacologically-augmented psychotherapy as an improved approach to treat trauma and anxiety-related disorders in a more efficient and persistent way promoting enhanced symptom remission and recovery.
Noradrenergic Regulation of Fear and Drug-Associated Memory Reconsolidation
Emotional and traumatic experiences lead to the development of particularly strong memories that can drive neuropsychiatric disorders, such as posttraumatic stress disorder (PTSD) and drug addiction. Disruption of these memories would therefore serve as a powerful treatment option, and targeting the pathologic emotional, but not declarative, component of a memory would be ideal for clinical intervention. Research reveals that after retrieval of a consolidated memory, the memory can be destabilized, and must then be reconsolidated through synaptic plasticity to allow subsequent retrieval. Disruption of reconsolidation-related plasticity would therefore impair specific, reactivated memories. Noradrenergic signaling strengthens synaptic plasticity and is essential for encoding the emotional components of memory. Consistent with this, investigations have now revealed that noradrenergic signaling is a critical mechanism for reconsolidation of emotional memories in rodent and human models. Here, we discuss these investigations and promising clinical trials indicating that disruption of noradrenergic signaling during reconsolidation may abolish the pathologic emotional, but not declarative, component of memories allowing alleviation of neuropsychiatric disorders including PTSD and drug addiction.
Other novel options:
Modulation of fear memory by dietary polyunsaturated fatty acids via cannabinoid receptors.
A Diet Enriched With Curcumin Impairs Newly Acquired and Reactivated Fear Memories.
